NURBN3030 Management of Deteriorating Patient Report Sample
Task Overview
Students will be randomly allocated one of four pre-determined topics that are common causes of patient deterioration. Students must then develop and submit a Mind Map focusing on the topic they have been allocated. Please see the Task Instructions chapter of this Moodle book to read about how you can identify which group you have been allocated to.
The four disease states (topics), all of which are common causes of patient deterioration, are:
1. Burns
2. Long Bone Fracture
3. Paediatric Asthma
4. Sepsis
Task Purpose
The aim of creating a Mind Map of the topic is to enable students to:
• Demonstrate an understanding of key concepts associated with patient deterioration,
• Explore the relationships between the pathophysiology, aetiology, clinical manifestations, and the presenting signs and symptoms,
• Prioritise and implement nursing interventions.
Task Instructions
Step 1: Check your topic allocation
Step 2: Research - Evidence of Best Practice
You are required to research and critically analyse your topic within the context of the deteriorating patient. You will identify primary concepts of the disease state; the basic concepts of the underlying pathophysiology (i.e., Asthma can be intrinsic or extrinsic etc); key principals in management; nursing assessments; and interventions for the disease state.
Step 3: Plan and Create your Mind Map
To create and refine your Mind Map, begin with the disease state as your central concept. This will be the focus of your Mind Map and most connections will be made with this. Branching off from this central concept, you will then address and include the following:
Pathophysiology: Identify the specific underlying pathophysiology of your topic and demonstrate your understanding of the disease progression toward patient deterioration.
Aetiology: Show your understanding of the causes associated with your topic by using connecting lines to branch out from the central idea, making make specific connections between the causes of the disease state and the underlying pathophysiology.
Clinical Manifestations: Introduce clinical manifestations and how these would present within physical assessment findings in the context of an acute presentation. Ensure that you present the expected assessment findings – for example: changes to perfusion should be described in terms of capillary refill, pulse pressure, skin colour/warmth etc. You should further link these with the underlying pathophysiology and the aetiology (causes of these clinical manifestations).
Nursing Assessments and Interventions: Identify priority nursing assessments and priorities of care for your topic. Include at least 3 nursing interventions that can be implemented by you as a graduate nurse to support the deteriorating patient presenting with this condition. Link these to pathophysiology, aetiology and clinical manifestations.
Management: Identify the management or treatment related to clinical manifestations including pharmacological interventions.
Referencing
For this assessment, you must use at least 7 current (within 5 - 7 years) peer-reviewed references in your paper to support your work. In-text citations for text and graphics must be included on the Mind Map. You must also include a reference list formatted using APA 7th Edition guidelines.
Solution
Introduction
The study on pediatric asthma will draw attention towards the intricate aspects of the disease while shedding light on the ability to justify collected information through literature support. Several sections have been made within the study for bringing about a clear structural guidance within the same.
Pathophysiology:
Pediatric asthma is a chronic inflammatory disease of the airways. Different factors are responsible for hyperreactivity of the airways and chronic inflammation that results in pediatric asthma. According to Pijnenburg et al. (2022), genetic, immunological factors and environmental are some factors related to the pathophysiology of pediatric asthma. This resulted in a tightness in the chest, obstacles in airways, breathlessness and other characteristics of pediatric asthma. This is the reason to effectively treat and manage a patient who is suffering from pediatric asthma, it is very important to understand the cellular mechanism that is responsible for it. Bronchoconstriction is one of the reasons for a pediatric asthma condition. The airway lumen is narrowed due to bronchoconstriction and this results in obstacles in the airways (Siora et al., 2024). Airways inflammation is another reason for a pediatric asthma condition. Within the environment, some triggers such as allergens or irritants are active in the airway mucosa. These are also resulted in pediatric asthma conditions. Mucous hypersecretion is also responsible for a pediatric asthma condition. The high amount of mucous secretion results in a block in the airways that leads to a pediatric asthma condition. The discussion highlighted that there is a need to effectively control inflammation and other cellular process that help in reducing pediatric asthma conditions.
Aetiology:
Genetic and environmental factors both are responsible for developing this disease within individuals, especially in children. This is referred to as the aetiology of pediatric asthma and this aspect needs to be understood to effectively manage pediatric asthma patients. According to Chatkin et al. (2022), environmental triggers such as allergens, smoke, air pollution, and respiratory infections are the aetiology of pediatric asthma. Within the environment, different types of allergens are presented such as dust mites, pollen, and others are the triggers for pediatric asthma. Tobacco smoke is one of the environmental factors that is also responsible for developing asthma in children. In children who are exposed to high amounts of tobacco smoke, it is noticed that the chances of getting asthma are high. Within the polluted air, different types of materials are presented that are responsible for pediatric asthma. Such as within the polluted air the high amount of nitrogen dioxide, ozone, particulate matter and others are responsible for developing asthma in children. Viral respiratory tract infections in children are responsible for developing asthma. Genetic predisposition is the other aetiology that is associated with pediatric asthma. It is noticed that if any parents have this disease, the children are also faced the similar issues. The discussion highlighted both factors such as genetic predisposition and environmental factors how responsible for developing pediatric asthma conditions for university assignment help.
Clinical Manifestations:
Different types of symptoms are noticed in individuals who are suffering from pediatric asthma. To effectively treat this issue at an early stage, recognising these symptoms is important. Within this part of the assignment, the discussion will be on the clinical manifestations of pediatric asthma.
Wheezing:
According to Lecerf & Prince (2022), this is one of the most crucial symptoms noticed within pediatric asthma patients. Due to the inflammation and bronchoconstriction, the airways are blocked which results in the high accumulation of airflow. This created high-pitch wheezing with musical sound. Environmental triggers or genetic factors are responsible for it.
Cough:
Coughing is another symptom that indicates a child may suffer from asthma. Hypersecretion of mucus or airway irritation results in cough and leads to asthma in children.
Dyspnea:
The condition in which an individual suffers from shortness of breath is called dyspnea. This is another symptom of pediatric asthma. With this condition, patients have felt chest tightness, difficulties in deep breathing and others.
The discussion highlighted how these symptoms are connected to the pathophysiology and aetiology of pediatric asthma.
Nursing Assessments and Interventions
According to the study of Mowbray et al (2020), there is a gap in knowledge regarding nursing assessments in a setting of paediatric emergency. However, through the study of Mowbray et al (2020), it has been noticed that the evaluation of nursing practitioners suggested 18 per cent paediatric patient presented for asthma care and the nursing assessments were achieved for the availability of nursing practitioners in time-sensitive quality measures of asthma. The nursing assessments further concentrate on understanding pathophysiology such as infections or allergens to inform measures of prevention. The exploration in terms of aetiology involves factors of the environment and familial predispositions.
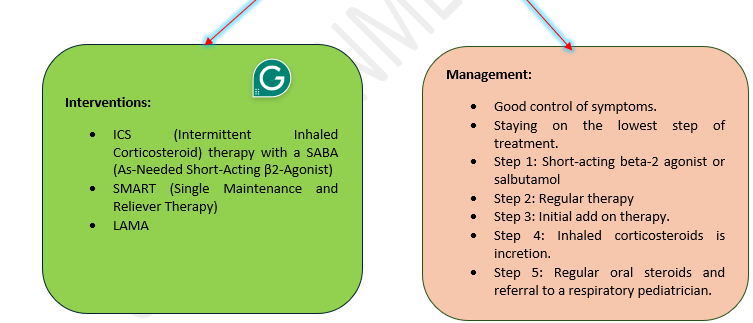
To manage paediatric asthma, relevant interventions encompass ICS (Intermittent Inhaled Corticosteroid) therapy with a SABA (As-Needed Short-Acting β2-Agonist) (Rodriguez-Martinez et al., 2022). In this approach, ICS is used according to the need of the patient with a SABA for quick relief. This intervention is essential for controlling symptoms. SMART (Single Maintenance and Reliever Therapy) is yet another intervention which combines both rescue medications and maintenance within a single inhaler (Van De Hei et al., 2022). For daily use, it includes a combination of ICS and LABA and during exacerbations as per the requirement. LAMA is also considered an essential intervention for children’s treatment who suffer with uncontrolled asthma, even after optimal therapy of ICS-LABA. To improve lung function among children and help in relaxing airway muscles, LAMA is a significant intervention (Pelaia et al., 2022).
Management
The aim of management regarding paediatric asthma is to successfully achieve good control of symptoms. Achieving this aim involves good attendance in schools, bounded limitation on daily activity, no disturbance in sleep routine, no exacerbations. Moreover, the SIGN (Scottish Intercollegiate Guideline Network), British Thoracic Society, and GINA (Global Initiative for Asthma) regularly review the management guidelines (Holden et al., 2018). Furthermore, the current aim of management is to control the symptoms while staying on the lowest step of treatment. The stepwise management involves 5 diverse steps. In step 1, short-acting beta-2 agonist or salbutamol is prescribed. In step 2, regular therapy of symptom prevention is done while using inhaler corticosteroids. Therefore, initial add on therapy is performed. In step 4, if the control rate is found to be poor, the dose of inhaled corticosteroids is increased. Finally, in step 5, regular oral steroids are offered, and the patient is referred to a respiratory pediatrician.
Mind Map

Conclusion
The intricacies of paediatric asthma along with the most effective interventions have been stated within the write-up and a descriptive Mind Map has been developed for clearer evaluation of personal understanding.
References:
Chatkin, J., Correa, L., & Santos, U. (2022). External environmental pollution as a risk factor for asthma. Clinical reviews in allergy & immunology, 62(1), 72-89. https://link.springer.com/article/10.1007/s12016-020-08830-5
Holden, K., Stewart , H., & Bonfield, A. (2018, October 22). Asthma - diagnosis - management - attacks. TeachMePaediatrics. https://teachmepaediatrics.com/respiratory/lower-respiratory-tract/asthma/
Lecerf, K., & Prince, B. T. (2022). Paediatric asthma-all that wheezes is not necessarily asthma-current diagnostic and management strategies. Current Opinion in Pulmonary Medicine, 28(3), 258-265. https://doi.org/10.1097/MCP.0000000000000874
Mowbray, F. I., DeLaroche, A. M., Parker, S. J., Jones, A., & Ravichandran, Y. (2020). Examining the clinical management of asthma exacerbations by nurse practitioners in a pediatric emergency department. International Emergency Nursing, 50, 100844. https://doi.org/10.1016/j.ienj.2020.100844
Pelaia, C., Crimi, C., Crimi, N., Ricciardi, L., Scichilone, N., Valenti, G., ... & Pelaia, G. (2022). Indacaterol/glycopyrronium/mometasone fixed dose combination for uncontrolled asthma. Expert Review of Respiratory Medicine, 16(2), 183-195. https://doi.org/10.1080/17476348.2021.2011222
Pijnenburg, M. W., Frey, U., De Jongste, J. C., & Saglani, S. (2022). Childhood asthma: pathogenesis and phenotypes. European Respiratory Journal, 59(6). DOI: 10.1183/13993003.00731-2021
Rodriguez-Martinez, C. E., Sossa-Briceño, M. P., & Garcia-Marcos, L. (2022). Use of inhaled corticosteroids on an intermittent or as-needed basis in pediatric asthma: a systematic review of the literature. Journal of Asthma, 59(11), 2189-2200. https://doi.org/10.1080/02770903.2021.2008430
Siora, A., Vontetsianos, A., Chynkiamis, N., Anagnostopoulou, C., Bartziokas, K., Anagnostopoulos, N., ... & Papaioannou, A. I. (2024). Small airways in asthma: From inflammation and pathophysiology to treatment response. Respiratory Medicine, 107532. https://doi.org/10.1016/j.rmed.2024.107532
Van De Hei, S. J., Poot, C. C., Van Den Berg, L. N., Meijer, E., Van Boven, J. F., Flokstra-de Blok, B. M., ... & Kocks, J. W. (2022). Effectiveness, usability and acceptability of a smart inhaler programme in patients with asthma: protocol of the multicentre, pragmatic, open-label, cluster randomised controlled ACCEPTANCE trial. BMJ open respiratory research, 9(1), e001400. https://doi.org/10.1136/bmjresp-2022-001400
Would you like to schedule a callback?

Highlights
Earn While You Learn With Us
Confidentiality Agreement
Money Back Guarantee
Live Expert Sessions
550+ Ph.D Experts
21 Step Quality Check
100% Quality
24*7 Live Help
On Time Delivery
Plagiarism-Free

 81 Isla Avenue Glenroy, Mel, VIC, 3046 AU
81 Isla Avenue Glenroy, Mel, VIC, 3046 AU



